

Background: In Acute Myeloid Leukemia (AML), identification of measurable residual disease (MRD) thresholds with clinical significance is still a matter of debate. For this purpose, multiparametric flow cytometry (MFC) is extensively employed for MRD quantification, due to high sensitivity (down to 1:10-3/10-5 cells) and wide applicability (up to 90% of cases). The identification of 20 clustered residual leukemic cells seems sufficient for the recognition of MRD presence (lower limit of detection [LOD]), whereas a cluster of 50 events may be the minimum threshold for the quantification of a cell population (lower limit of quantitation [LOQ]), provided a sufficient denominator of relevant events (500'000-1'000'000) is acquired.
Methods: Using a MFC assay, we assessed the predictive power of a threshold calculated applying the criteria of LOD and LOQ on 261 intensively treated AML patients enrolled in the GIMEMA AML1310 prospective trial.According to the protocol design, patients with a bone marrow residual leukemic cells count (RLCc) equal or above 0.035% of the total no. of mononuclear (MNC) cells qualified as MRDpos,, whileusing LOD and LOQ, we selected the following categories of patients: 1) LODneg if RLCc was below LOD (20x100/total no. of events); 2) LODpos-LOQneg if RLCc was between LOD and LOQ; and 3) LOQpos if RLCc was above LOQ (50x100/total no. of events).
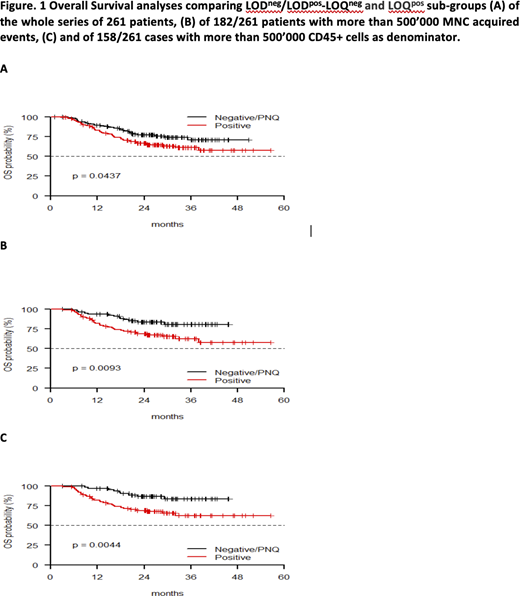
Results: The ELN target of 500'000 events was reached in 182/261 (69.6%) patients. Overall, using the predefined AML1310 protocol MRD threshold, 154 (59%) and 107 (41%) were MRDneg and MRDpos, respectively, whereas 74 (28.4%), 43 (16.5%) and 144 (54.4%) patients were classified as LODneg, LODpos-LOQneg and LOQpos, respectively. Two-year overall survival (OS) was 75.4% vs. 79.8% vs. 66.4% for LODneg, LODpos-LOQneg and LODpos, respectively (p=0.1197), and 74.5% vs. 66.4% according to AML1310 protocol 0.035% threshold for MRDneg and MRDpos patients, respectively (p=0.3521). Due to superimposable outcome, LOD-LOQneg and LODpos-LOQneg categories were combined. Accordingly, LODneg/LODpos-LOQneg and LOQpos groups clearly differed in terms of OS (77% vs. 66.4%, p=0.0437) [FIGURE 1A]. Such a figure was challenged in multivariate analysis (p=0.048, HR 0.628, 95% CI 0.396-0.997) that confirmed the independent role of LOD-LOQ approach in influencing OS.
To enhance the predictivity of LOD-LOQ estimate, we then focused on samples acquisition of which passed the 500'000 events, according to ELN guidelines. Among 182/261 (69.7%) cases with > 500'000 MNC events as denominator, LODneg/LODpos-LOQneg and LOQpos subgroups were clearly distinct in terms of OS (2-years OS of 83.5% vs. 69.4%, p=0.009). [FIGURE 1B]
Similarly, also when selecting those patients (158/261 [60.5%]) whose acquisition passed 500'000 CD45+ events, LODneg/LODpos-LOQneg and LOQpos showed a different behavior with 2-years OS of 86.7% vs. 69.0%, respectively (p=0.004). [FIGURE 1C]
Finally, when considering the interaction of the 3 LOD-LOQ categories with possible post-remissional strategies, LODneg/LODpos-LOQneg patients submitted to autologous stem cell transplant showed the best 2-years OS (88.9%) as compared to all the other categories (allogeneic stem cells transplant and no graft-based treatments) (p=0.026).
Summary/Conclusion: In conclusion, the use of LOD-LOQ method results in a more sensitive detection of MRD that, in turn, translates in a more accurate recognition of patients with different prognosis. Actually, such an approach allowed to dissect even further the category of patients called MRDneg according to the AML1310 protocol definition, since MRDneg subjects who belonged to a "true negative" LOD-LOQ sub-group [LODneg/LODpos-LOQneg] had a better outcome than the other MRDneg ones. This MRD approach could serve as a useful tool to personalize post-remission strategy in intensively treated AML patients, through selection of high-quality remission patients who may benefit from less intensive post-consolidation therapies.
Voso:Bristol Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Venditti:Novartis: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company); Pfizer: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Speakers Bureau; Amgen: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company); Jazz: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company); AbbVie: Consultancy, Honoraria, Other: TRAVEL, ACCOMODATIONS, EXPENSES (paid by any for-profit health care company); Janssen: Consultancy, Honoraria, Other: TRAVEL, ACCOMODATIONS, EXPENSES (paid by any for-profit health care company).

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal